Introduction
Physiotherapy in Toronto for Knee
Welcome to In Balance Physiotherapy's patient resource about Tibial Osteotomy.
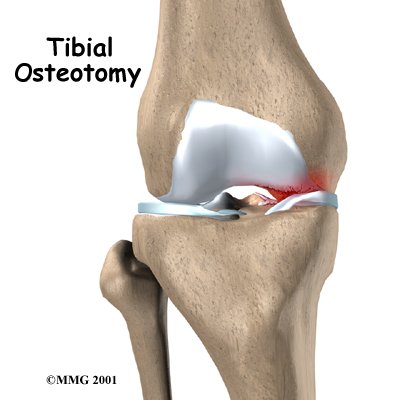
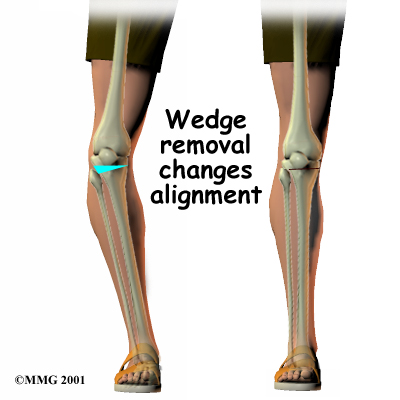
Knee osteoarthritis often affects only one side of the knee joint. When this occurs, realigning the angle made between the bones of the leg can shift your body weight so that the healthy side of the knee joint takes more of the stress. The procedure to realign the angles of the lower leg is called a proximal tibial osteotomy.
This guide will help you understand:
- what your surgeon hopes to achieve with the procedure
- what happens during the surgery
- what to expect after your operation
Related Document: In Balance Physiotherapy's Guide to Osteoarthritis of the Knee
Anatomy
Which parts of the knee are involved?
The knee joint is formed where the thighbone (femur) meets the shinbone (tibia). Two bony knobs on the end of the femur, called condyles, sit on the top surface of the tibia. The inside condyle (the one closest to the other knee) is called the medial femoral condyle. The lateral femoral condyle is on the outer half of the femur (farthest from the other knee). The top of the tibia bone forms a flat surface called the tibial plateau.
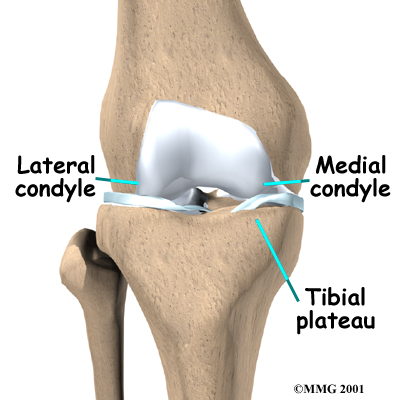
The knee is divided into two halves, or compartments. The medial compartment is the inside half of the knee and is formed by the connection of the medial femoral condyle and the tibial plateau. The lateral compartment is the outside half of the knee and is formed by the connection of the lateral femoral condyle and the tibial plateau.
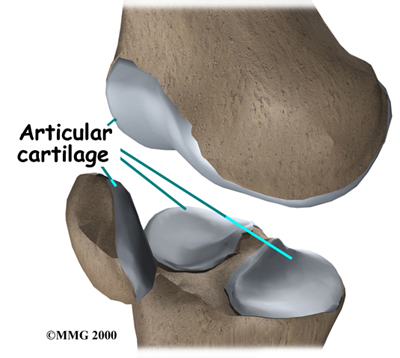
covers the ends of bones. It has a smooth, slippery surface that allows the bones of the knee joint to slide over each other without rubbing. This slick surface is designed to minimize pressure and friction as you move.
Related Document: In Balance Physiotherapy's Guide to Knee Anatomy
Knee Anatomy Introduction
Rationale
What does the surgeon hope to achieve with surgery?
Osteoarthritis of the knee sometimes affects one side of the knee far more than the other. While either side can suffer greater damage, usually the inside half of the knee joint (the medial compartment) is more affected. When this uneven damage occurs to one side of the knee, the other side may still have good cartilage on the joint surfaces.
In some cases, surgery to realign the angles in the lower leg can result in shifting pressure to the other, healthier side of the knee. The goal is to reduce the pain and delay further degeneration in the weaker half of the knee.
This procedure is most often used for younger, active patients and for those who have osteoarthritis in only one side of their knee joint. This operation may increase the life span of the joint and prolong the time before a knee replacement surgery becomes necessary.
Preparation
How should I prepare for surgery?
The decision to proceed with surgery must be made jointly by you and your surgeon. You need to understand as much about the procedure as possible. If you have concerns or questions, you should talk to your surgeon.
Once you decide on surgery, you need to take several steps. Your surgeon may suggest a complete physical examination by your regular doctor. This exam helps ensure that you are in the best possible condition to undergo the operation.
On the day of your surgery, you will probably be admitted to the hospital early in the morning. You shouldn't eat or drink anything after midnight the night before. The amount of time you spend in the hospital varies and depends on how quickly you recover.
Surgical Procedure
What happens during the operation?
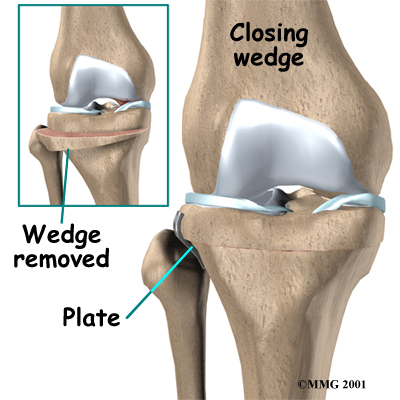 There are two methods to realign the knee joint. One involves taking out a wedge of bone; the other involves adding a wedge of bone. Any operation for cutting through a bone is called an osteotomy. In a closing wedge osteotomy, the surgeon cuts though the tibia on the lateral side, removes a wedge of bone, and pins the open edges together. In an opening wedge osteotomy, the surgeon cuts though the tibia on the medial side and opens a wedge, adding a bit of bone graft to hold the wedge open.
There are two methods to realign the knee joint. One involves taking out a wedge of bone; the other involves adding a wedge of bone. Any operation for cutting through a bone is called an osteotomy. In a closing wedge osteotomy, the surgeon cuts though the tibia on the lateral side, removes a wedge of bone, and pins the open edges together. In an opening wedge osteotomy, the surgeon cuts though the tibia on the medial side and opens a wedge, adding a bit of bone graft to hold the wedge open.
Closing Wedge Osteotomy
In the , an incision is made in the lateral side of the knee to allow the surgeon to see the upper end of the tibia. Care is taken to protect the nerves and blood vessels that travel across the knee joint.
Once the tibia bone is exposed, two cuts are made through the upper tibia in the shape of a wedge. The surgeon uses either X-rays or a fluoroscope, a special kind of X-ray machine that casts images on a fluorescent screen, to make sure the wedge is the right size and is placed correctly.
The surgeon takes out the wedge, and the two sides of the tibia are brought closer together and held in position with a metal plate or pins. This and helps straighten the alignment of the knee. After fixing the two edges of bone with a plate or pins, the surgeon stitches the skin together, and the leg is placed in a padded splint to protect the knee joint.
Opening Wedge Osteotomy
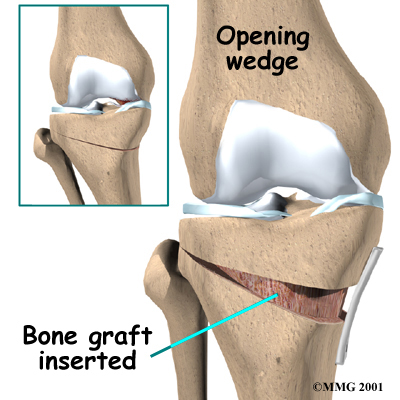
In the , an incision is made in the medial side of the knee. Again, care is taken to protect the nerves and blood vessels that travel across the knee joint.
Once the tibia bone is exposed, one cut is made through the upper tibia. A fluoroscope or X-rays are used to make sure the cut is in the right place.
After the bone is cut, the two sides of the tibia are separated to form a wedge-shaped opening.
This opening is then filled with bone graft. The bone graft is usually taken from pelvis bone, through an incision in the side of your hip.
The bone graft is held in position with a metal plate or pins.
After fixing the two edges of bone with a plate or pins, the surgeon stitches the skin together, and the leg is placed in a padded splint to protect the knee joint.
Complications
What might go wrong?
As with all major surgical procedures, complications can occur. This document doesn't provide a complete list of the possible complications, but it does highlight some of the most common problems. Some of the most common complications following tibial osteotomy are:
- anesthesia complications
- thrombophlebitis
- infection
- scar tissue formation
- nonunion of the bones
Anesthesia Complications
Most surgical procedures require that some type of anesthesia be done before surgery. A very small number of patients have problems with anesthesia. These problems can be reactions to the drugs used, problems related to other medical complications, and problems due to the anesthesia. Be sure to discuss the risks and your concerns with your anesthesiologist.
Thrombophlebitis (Blood Clots)
Thrombophlebitis, sometimes called deep venous thrombosis (DVT), can occur after any operation, but is more likely to occur following surgery on the hip, pelvis, or knee. DVT occurs when blood clots form in the large veins of the leg. This may cause the leg to swell and become warm to the touch and painful. If the blood clots in the veins break apart, they can travel to the lung, where they lodge in the capillaries and cut off the blood supply to a portion of the lung. This is called a pulmonary embolism. (Pulmonary means lung, and embolism refers to a fragment of something traveling through the vascular system.) Most surgeons take preventing DVT very seriously. There are many ways to reduce the risk of DVT, but probably the most effective is getting you moving as soon as possible after surgery. Two other commonly used preventative measures include:
- pressure stockings to keep the blood in the legs moving
- medications that thin the blood and prevent blood clots from forming
Infection
Following surgery, it is possible that the surgical incision can become infected. This will require antibiotics and possibly another surgical procedure to drain the infection.
Scar Tissue Formation
The most common complication after a tibial osteotomy is the formation of scar tissue in the joint below the kneecap. Bleeding and swelling from the surgery can cause the body to form scar tissue. When scar tissue builds up just below the kneecap, the knee can't straighten completely. When this happens, another operation may be required to remove the scar tissue.
Nonunion of the Bones
Sometimes the two bone edges do not heal as planned. This is called a nonunion. This condition requires another operation to add bone graft and perhaps additional metal plates or pins. The bones need to be completely immobilized to fuse, or heal together firmly, so an external fixator may be needed to help hold the bones in position as they heal. The external fixator is worn over the skin and connects to the metal pins to hold them firmly in place. Because the bone of the upper tibia is wide and has a good blood supply, nonunion is rare.
Continued Pain
In some cases the tibial osteotomy simply does not achieve the results expected. This can occur due to more advanced osteoarthritis in other areas of the joint, especially in the cartilage behind the kneecap. If you continue to have pain or do not achieve the results that you expect from the operation, the next step is usually to replace the knee joint with an artificial joint.
Related Document: In Balance Physiotherapy's Guide to Artificial Joint Replacement of the Knee
After Surgery
What happens after surgery?
Your surgeon may have you use a continuous passive motion (CPM) machine immediately after surgery to help the knee begin moving and to alleviate joint stiffness. The machine straps to the leg and continuously bends and straightens the joint. This motion is thought to reduce stiffness, ease pain, prevent blood clots from forming, and prevent extra scar tissue from forming inside the joint.
Along with the CPM, you may be seen by a physiotherapist to maximize your range of motion. As your condition stabilizes, your physiotherapist will also help you up for a short outing using your crutches or your walker.
Most patients are able to go home after spending one or two days in the hospital. You'll be on your way home when you can demonstrate a safe ability to get in and out of bed, walk up to 75 feet with your crutches or walker, go up and down stairs safely, and access the bathroom. It is also important that you regain a good muscle contraction of the quadriceps muscle in the thigh and that you gain improved knee range of motion.
A tibial osteotomy in the best of circumstances is probably only temporary. It is thought that this operation buys some time before a total knee replacement becomes necessary. The benefits of the operation usually last for five to seven years if successful.
Our Rehabilitation
What should I expect during my rehabilitation?
You will probably wear a knee brace for up to six weeks after surgery to protect the knee joint as you recover. Your stitches will normally be removed in 10 to 14 days. Although the time required for rehabilitation varies, recovery after a tibial osteotomy typically takes two to three months.
During your recovery period, you should use your walker or crutches as instructed by our physiotherapist. If you had a closing wedge osteotomy, you probably won't have to limit how much weight you place on your foot. But with an opening wedge procedure, you'll need to protect the healing bone graft by only placing the toes of the operated leg on the floor when you walk. Your surgeon will take a follow-up X-ray to see when the graft is safe for you to begin putting more weight down when you walk. This is usually six to eight weeks after surgery.
Your physiotherapist can begin assisting you with treatment shortly after surgery. Our physiotherapist may use heat, ice, or electrical stimulation if you have swelling or pain. We may also use hands-on stretches and show you exercises to improve knee range of motion. Then strength exercises will be used to address key muscle groups including the buttock, hip, thigh, and calf muscles. Endurance can be achieved through stationary biking, lap swimming, and using an upper body ergometer (upper cycle).
Our physiotherapists sometimes treat patients in a pool. Exercising in a swimming pool puts less stress on the knee joint, and the buoyancy lets you move and exercise easier. Once you've gotten your pool exercises down and the other parts of your rehab program advance, we may instruct you in an independent program.
When you are safe in putting full weight through the leg, our physiotherapist can choose several types of balance exercises to further stabilize and control your knee.
Finally, we will utilize a select group of exercises to simulate day-to-day activities, such as going up and down steps, squatting, rising on your toes, and bending down. Other specific exercises may then be chosen to simulate work or hobby demands.
Many patients have less pain and better mobility after a tibial osteotomy procedure. Our physiotherapist will work with you to help keep your knee joint healthy for as long as possible. This may require that you adjust your activity choices to keep from placing too much strain on your knee.
At In Balance Physiotherapy, our goal is to help you improve knee range of motion, maximize strength, and improve your ability to do your activities. When your recovery is well under way, regular visits to our office will end. Although we will continue to be a resource, you will be in charge of doing your exercises as part of an ongoing home program.
In Balance Physiotherapy provides services for physiotherapy in Toronto.
Portions of this document copyright MMG, LLC.